
Legacy: The Dual-Barrier Reality
For 25 years, the medical community viewed Cerebral Palsy through a single lens: a static brain injury. The NeuroLoop Protocol reveals a more complex truth. The “barrier” to a cure isn’t just the scar in the brain—it is the Secondary Biological Abyss in the muscle.
In the CLEAR phase, we dismantle two distinct walls:
- The Central Barrier: The Glial Scar and Myelin Debris in the brain.
- The Peripheral Barrier: The “Accelerated Aging” and Fibrosis in the muscle.
Legacy Position:
- Systemic Suppression: Reliance on medications like Baclofen to manage spasticity, causing global CNS suppression and cognitive clouding that interrupts critical developmental windows.
- The Glial Scar & Diffuse Gliosis: Viewed as an impenetrable wall in focal injuries or a toxic “honeycomb” in deep gray matter, leaving clinicians with no tools to dismantle these inhibitory zones.
- Myelin Debris: A failure to address the “biological poison” left behind after HIE, which prevents the brain’s natural repair cells from functioning.
- Static Treatment: Use of high-dose steroids and basic physical therapy that managed symptoms but failed to repair the underlying biological “wiring.”
1. Central Restoration: Brain Scar & Myelin Repair
Mapping to the Deep Gray Matter (HIE) and White Matter (PVL)
The CLEAR phase transitions the Neuroloop from mapping to active structural remodeling. Whether addressing focal loss in the Basal Ganglia and Thalamus (HIE) or the diffuse white matter injury of Periventricular Leukomalacia (PVL), we move beyond masking symptoms to targeting the root cause of neurological dysfunction.
- Enzymatic Detoxification: Dissolving the “glue” of the glial scar (CSPGs) and Perineuronal Nets (PNNs) to re-open the critical period for learning, utilizing targeted delivery of chondroitinase.
- OPC Activation & White Matter Recovery: Leveraging small-molecule therapeutics to “wake up” dormant Oligodendrocyte Progenitor Cells (OPCs), triggering the active production of new myelin to repair the Internal Capsule and other vital relay tracts.
- Restoring Conduction Fidelity: By rebuilding the fatty insulation (myelin) around exposed axons, we ensure electrical impulses travel at the precise velocities required for functional movement and complex thought.
- Scaffold Integration & Volume Repair: Deploying bio-resorbable structures to provide a 3D matrix in areas of cystic loss, stabilizing the architecture of the deep gray matter for future integration.
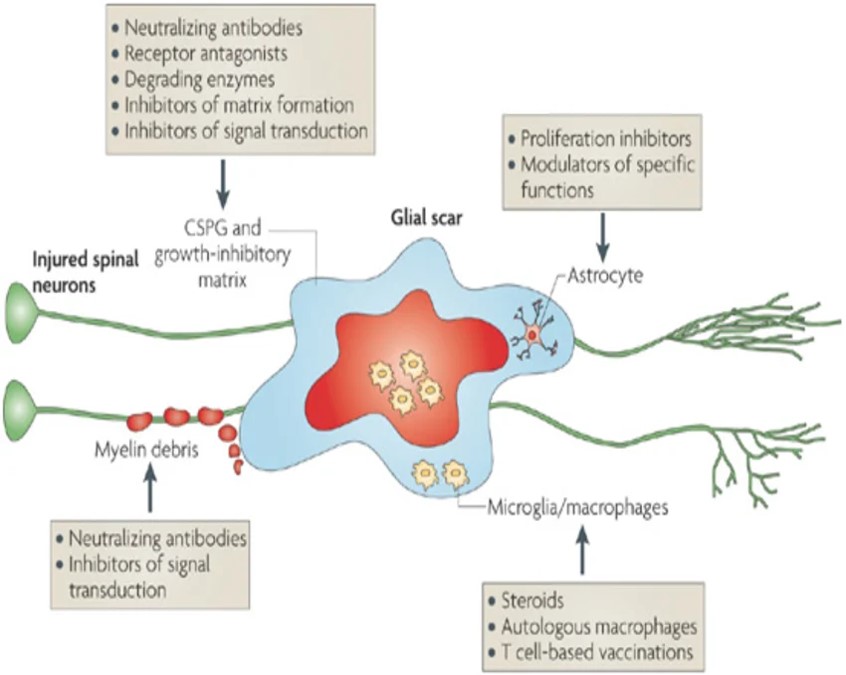
Image uploaded by Asya Rolls
2. Peripheral Restoration: Reversing Muscle “Aging”
New Learning for 2026: Muscle as a Degenerative Clock
Recent research (Horwath et al., 2026; Stewart et al., 2026) proves that CP muscle is not just “weak”—it is biologically aged. Without intervention, the muscle enters a “Toxic Abyss” characterized by:
- Cellular Senescence: “Zombie cells” that leak inflammatory toxins (SASP), preventing growth.
- Stem Cell Exhaustion: A 40–70% reduction in the satellite cells needed for repair.
- Fibrotic Locking: Stem cells being “reprogrammed” to build internal scar tissue (contractures) instead of healthy muscle.
3. The CLEAR Pharma “Audit” Toolkit
| Tier | Intervention | Primary Target | NeuroLoop Role |
|---|---|---|---|
| Tier 1: Shield | N-Acetylcysteine (NAC) | Oxidative Stress | Environmental Cleanup: Neutralizes the “toxic smoke” (SASP) before it causes permanent aging. |
| Tier 2: Unlock | Losartan | TGF-beta / Fibrosis | Chemical Debridement: Stops stem cells from turning into scars, breaking the “physical lock” of contractures. |
| Tier 3: Purge | Senolytics | “Zombie” Cells | Molecular Reset: Selectively removes aged cells to refresh the regenerative environment. |
4. The “Tightrope” Analogy: Why Daily Movement is Non-Negotiable
Think of a child with CP as walking a Functional Tightrope.
- On the rope, they are moving, learning, and keeping the “toxic smoke” at bay.
- If they stop moving—even for a few weeks—they fall off the rope into the “Toxic Abyss.”
- Once in the abyss, the muscles become so inflamed and scarred that standard physical therapy can no longer reach them.
Our Goal: Use the CLEAR toolkit to pull the child back up onto the tightrope. Once the “biological noise” is cleared, our high-intensity movement protocols (SYNC) can finally rewire the system.
2026 Frontier Research Targets
- SASP Speedometers: Tracking circulating proteins (GDF15, IL-6) to objectively measure if a child’s “biological clock” is slowing down.
- Liquid Biopsies: Using exosome cargo to monitor muscle health without invasive surgery.
- Contracture Redefinition: Moving from “short muscles” (surgical target) to “fibrotic reprogramming” (pharmacological target).
“We are clearing the ruins to build the future.”
Cutting-edge research for 2025–2026 is shifting away from viewing the HIE scar as a simple “wall” and toward treating it as a chemically active barrier that can be enzymatically “reprogrammed.”
1. Key Research Hubs & Scientists (2025-2026)
- UMC Utrecht (The Netherlands) – Dr. Cora Nijboer & The NEOREPAIR Project:
- This group is arguably at the global forefront of neonatal brain repair.
- 2025-2026 Focus: They are moving beyond simple neuroprotection to regenerative strategies. Their iSTOP-CP phase II clinical study (launching October 2025) uses intranasal stem cells to modulate the environment and repair neural networks.
- Specific Insight: They are investigating how to “unravel the neuroregenerative mechanisms” of extracellular vesicles to clear the toxic environment in HIE-injured brains.
- University of Toronto / Sunnybrook Research Institute – The Shoichet Lab:
- 2025 Breakthrough: They recently redesigned Chondroitinase ABC (ChASE37) to be significantly more stable than the native version.
- Technique: They use an injectable hydrogel (CMC-bp) to provide prolonged, site-specific release of the enzyme. This is critical for HIE because it allows the enzyme to penetrate the deep nuclei (Basal Ganglia/Thalamus) rather than being washed away.
- University of Florida / Case Western – Silver & Bradbury Legacy Groups:
- While the 2002/2004 papers are “legacy,” their current descendants are focusing on PNN Modulation.
- 2026 Research: They are exploring how PNNs specifically in the Thalamus inhibit plasticity. By using enzymatic debridement, they aim to “re-open” the critical period of development, allowing the HIE-injured brain to “re-learn” motor functions.
- Enzyme Engineering (ChASE37): Native Chondroitinase is fragile and dies quickly at body temperature. The 2025-2026 “frontier” is Redesigned Enzymes with point mutations that allow them to stay active for weeks, providing a sustained “cleanup” of the HIE-injured site.
- Nanoscale Scaffold Integration: Researchers are moving toward bio-resorbable structures that don’t just “clear” the scar but fill the cystic voids (common in severe HIE) with a matrix that supports new growth.
- Intranasal Delivery: A major push in 2025 is bypassing the blood-brain barrier via the nose. This allows for repeated, less-invasive delivery of enzyme-stabilized nanoparticles or stem-cell-derived vesicles directly to the central CNS regions like the Thalamus.
- Neuren Pharmaceuticals: Developing NNZ-2591, a synthetic analog of brain peptides targeted specifically at HIE to improve the underlying biological landscape.
- Halozyme: Recently acquired technologies (2025-2026) focused on microparticulate delivery systems that could be adapted for sustained enzymatic release in the brain.
| Research Target | Primary Mechanism | 2025-2026 Status |
|---|---|---|
| Glial Scar (CSPGs) | ChASE37 + Hydrogel | Pre-clinical / Moving to human cell assays |
| Deep Gray Repair | Intranasal Stem Cells (EVs) | Phase II Clinical (iSTOP-CP) |
| Signal Speed (PLIC) | Small-molecule OPC activators | Early pipeline (Neuren/NNZ-2591) |
Tech Glossary
- Glial Scar / Diffuse Gliosis: A dense physical and chemical barrier formed by astrocytes following HIE that inhibits regrowth and locks circuits into a non-functional state.
- Oligodendrocyte Progenitor Cells (OPCs): The “reserve” cells of the brain that, when activated, transform into mature cells capable of repairing damaged myelin in HIE and PV
- CSPGs & PNNs: Inhibitory molecules and “nets” that stabilize the scar and stop nerve fibers from regenerating or forming new, healthy connections.
- Internal Capsule (PLIC): A critical white matter “highway” often damaged in HIE; its remyelination is the primary goal for motor restoration.
- Remyelination: The process of restoring the protective fatty sheath around nerve fibers to resume high-speed, high-fidelity signal conduction.
- Axonal Denudation: The loss of myelin that leaves a nerve fiber exposed and vulnerable to degradation—a hallmark of both PVL and chronic HIE.
Scholarly Citations
| 1.Single cell analysis of muscle contracture in cerebral palsy reveals pro-fibrotic and anti-myogenic stem cell populations with altered cell-cell interactions Madison Stewart, Lin-Ya Hu, Taryn Loomis, Sarah E Brashear, Lizbeth M De La Torre, Anas Mohamed Sulthan, Marie Villalba, Jon R Davids, Yue Wang, Vedant A Kulkarni, Lucas R Smith Am J Physiol Cell Physiol – 2026 Apr 23 (Online ahead of print) PMID: 42021719 |
- 29.Does Time Tick Faster in Cerebral Palsy? Accelerated Aging as a Framework for Skeletal Muscle Dysfunction Oscar Horwath, Sebastian Edman, Sudarshan Dayanidhi, Davis Englund, Mark D Peterson, Ferdinand von Walden FASEB J 2026 Mar 31;40(6):e71653 PMID: 41806256
- Silver, J., & Miller, J. H. (2004). Regeneration beyond the glial scar. Nature Reviews Neuroscience.
- Franklin, R. J. M., & Gallo, V. (2014). “The biology of CNS remyelination.” Nature Reviews Neuroscience.
- Bradbury, E. J., et al. (2002). Chondroitinase ABC promotes functional recovery after spinal cord injury. Nature.
- Volpe, J. J. (2009). The encephalopathy of prematurity—brain injury and impaired brain development. Lancet Neurology. (Addressing PVL/White matter nuances).




