
Discover Step Zero of the NeuroLoop Protocol. Learn how the NeuroLoop Stability Index (NL-SI) automates non-invasive airway and autonomic stabilization to prevent systemic exhaustion and unlock cortical neuroplasticity.
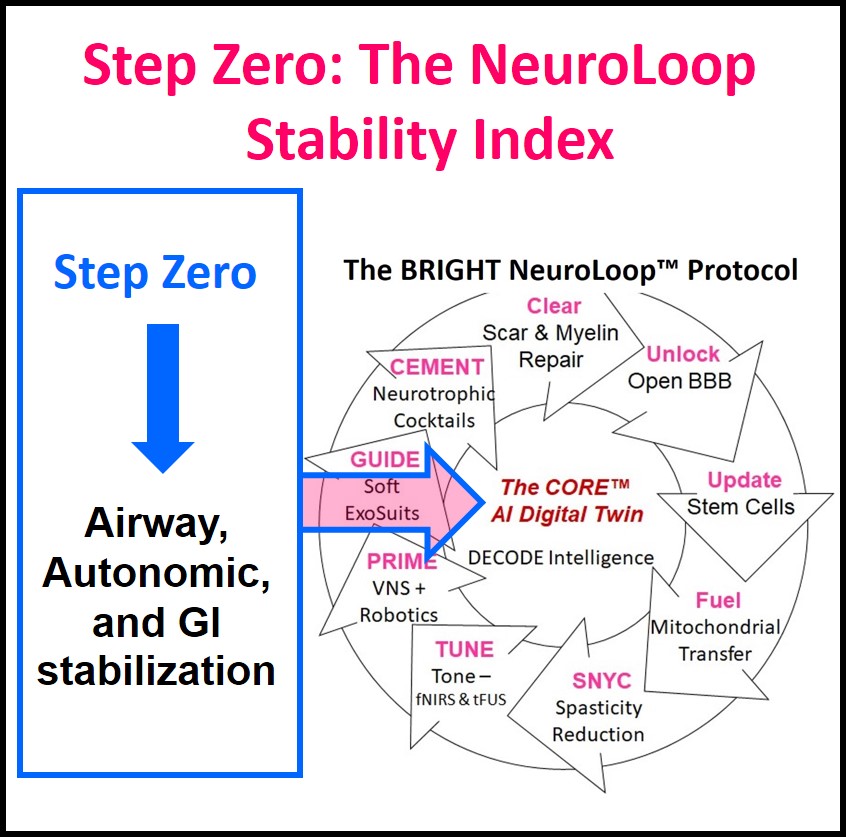
STEP ZERO: The NeuroLoop Stability Index (NL-SI)
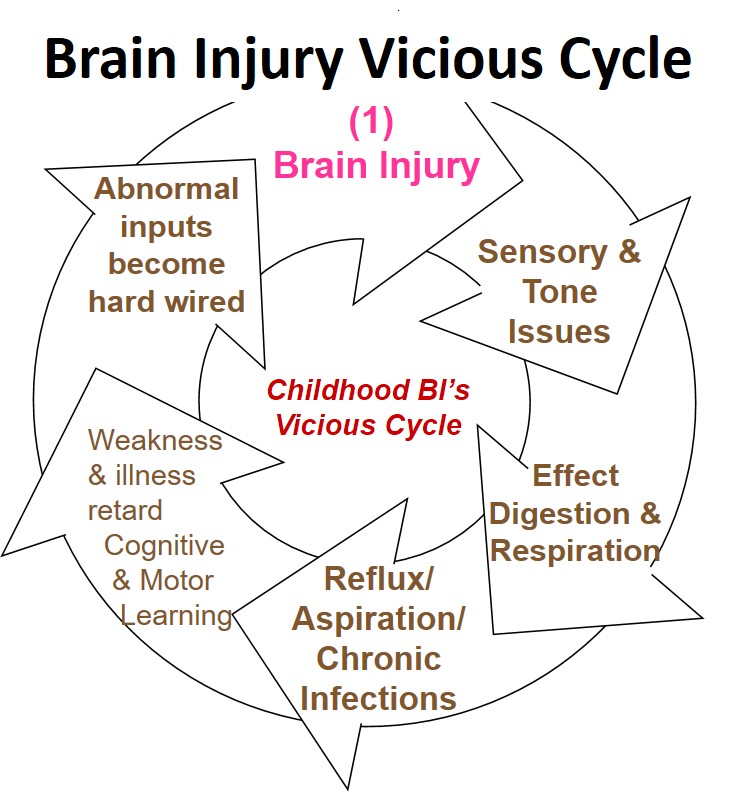
CP/Brain Injury is static correct? … so why do victims get worse? Stopping the “Brain Injury Vicious Cycle” by Stabilizing the Body’s Core Systems
1. The Paradigm Shift: Why We Begin at Step Zero
In traditional pediatric neurology, cerebral palsy (CP) and hypoxic-ischemic encephalopathy (HIE) are often treated purely as movement or muscle problems. Therapy usually reacts to the symptoms by focusing on tight muscles, stiff joints, and braces.
The BRIGHT Cerebral Palsy Cure Project looks at this differently. Human movement is not just a command sent from a damaged brain to a muscle. It is the result of how the entire body works together. The brain, nervous system, lungs, and gut are completely connected. Applying Dynamic Systems Theory (DST), human movement is not a pre-programmed command from a damaged motor cortex; it is an emergent property of a complex, highly integrated, self-organizing system. The brain, the peripheral nervous system, the airway, and the gastrointestinal (GI) tract are completely continuous.
Learning new movements is an incredibly high-energy task for a child’s brain. If a child’s body is constantly struggling just to breathe or digest food safely, their brain stays trapped in a survival loop.
Step Zero: The Stability Index is our proposed starting point. A child cannot focus their brain’s limited energy on learning to control their hands or feet if their entire nervous system is exhausted by the daily work of staying alive. Step Zero does not focus on muscles. Instead, its goal is to quiet down the background stress in the lungs and gut, creating a stable baseline so the brain is actually ready for neuroplastic learning.
2. The Scientific Advisory Board Foundation: Concepts from BRIGHT’s SAB
The design of Step Zero does not come from speculation; it is built directly upon the concepts pioneered by members of the BRIGHT Scientific Advisory Board (SAB).
Dynamic Systems Theory: The base rests upon Dr. Esther Thelen, whose work in Dynamic Systems Theory proved that motor patterns emerge from the real-time interaction of multiple subsystems. Her research showed that infant movement develops through the interaction of many body systems (strength, sensory feedback, and internal comfort). If one system is under massive stress, it acts as a roadblock that freezes overall progress. In severe CP/HIE, the ultimate roadblocks are often the airway and the digestive tract. When a child constantly struggles with choking, low oxygen, or severe reflux pain, their body hits a metabolic limit. We cannot retrain the brain if the body’s baseline is failing. Step Zero aims to fix these core roadblocks first.
Under Thelen’s framework, if a single subsystem is restricted or highly stressed, it acts as a rate limiter that locks the entire system into a maladaptive state. In severe CP/HIE, the ultimate rate limiters are the upper airway and the gastrointestinal tract. When a child experiences chronic micro-aspiration, oxygen desaturation, or severe visceral pain, the homeostatic subsystem is pushed to its absolute limit.
According to DST, you cannot alter the emergent behavior of the motor cortex by simply moving a child’s legs if the metabolic baseline is failing. Step Zero modifies these core boundary conditions first, removing the physiological constraints so that the Core AI can effectively retrain the motor system.
Cellular Stress: This systemic limit is reinforced by the cellular insights of Dr. Michael V. Johnston, whose foundational work on neonatal neuroprotection demonstrated how hypoxia-ischemia triggers an abnormal accumulation of intracellular calcium and metabolic stress cascades that destroy cellular homeostasis. Step Zero actively mitigates this cellular drain to protect vulnerable tissue.
Neurological Noise: Furthermore, Dr. Jonathan Mink’s deep mapping of basal ganglia physiology and the mechanisms of dystonia guides how the protocol identifies “overflow” muscle activation and tonic storms. If a child is in visceral pain, the basal ganglia’s gating mechanism fails, flooding the system with involuntary motor noise.
Filtering Signals: To capture these volatile biological signals, the mathematical constraints utilize the concepts of Dr. Nathan Urban, whose computational neuroscience research models how the brain transforms, filters, and processes sensory inputs. By applying computational de-noising and signal-transformation algorithms, the Core AI can separate a child’s true motor intent from the background chaos of autonomic stress.
Focusing on Potential: Finally, the entire protocol is grounded by the clinical advocacy of Dr. Janice Brunstrom, whose personal and professional life dedicated to intensive cerebral palsy rehabilitation underscores that structural limitations must never obscure a child’s absolute functional potential.
3. Real-World Examples of Systemic Collapse: The Tragic Proof of the Step Zero Law
Standard clinical practice often fails because it ignores the systemic nature of neurological injuries. Individuals with severe brain or spinal cord lesions rarely die from the primary injury to the nervous tissue; they succumb to the cascade of secondary autonomic, airway, and visceral failures.
Case Study 1: Christopher Reeve
Pioneering advocate Christopher Reeve sustained a catastrophic C1-C2 spinal cord injury, completely severing the connection between his brainstem and voluntary motor pathways. Yet, his death at age 52 was not caused by paralysis. Reeve died from systemic infection, sepsis, and subsequent multi-organ failure originating from an infected pressure ulcer—a direct result of a compromised autonomic circulatory loop, impaired tissue perfusion, and unmanaged sensory-motor feedback. His underlying biological platform collapsed under the weight of chronic, low-grade autonomic strain.
Case Study 2: Zain Nadella
Zain Nadella, son of Microsoft CEO Satya Nadella, was born with severe spastic cerebral palsy caused by intrauterine asphyxia (HIE). Throughout his 26 years of life, his primary battle was not the inability to walk; it was the relentless, exhausting drain of secondary systemic complications. Zain’s clinical trajectory was defined by progressive muscle spasticity, severe micro-aspiration, gastrointestinal gastroparesis, and chronic respiratory exhaustion. His system was locked in a constant, high-energy struggle to maintain basic respiration and airway protection, depleting the metabolic reserves required to support significant neuroplastic progression.
Both cases illustrate the Step Zero Law: The visceral, autonomic, and respiratory subsystems dictate survival and control the metabolic gateway to the brain. The NeuroLoop Protocol implements Step Zero as a mandatory gatekeeper to honor these lessons, to break the viscous cycle of brain injury the core anatomic functions must be stabilized.
4. How the Proposed NeuroLoop Stability Index (NL-SI) Will Work
To turn these ideas into practical tools, we are designing a real-time objective score called the NeuroLoop Stability Index (NL-SI).
Once built, this system will use cameras, audio sensors, and wearable monitors to calculate a continuous safety score from 0 to 100. Below a certain threshold number, the risks for spiraling downward outweigh the forces for stability or improvement. It is like walking on the edge of a cliff and a victim must always be far enough from the edge to not fall. The Stability Index score will suggest non-invasive treatments, and allow for an objective measurement how close a victim is to the edge of the cliff.
[ NEUROLOOP STABILITY INDEX (NL-SI) ]
│
┌───────────────────────────┼───────────────────────────┐
▼ ▼ ▼
[ AIRWAY VECTOR ] [ AUTONOMIC VECTOR ] [ VISCERAL VECTOR ]
• Swallow/Respiration Phase • Heart Rate Variability (HRV)• Visceral Pain Cues
• Laryngeal Acoustics • Sympathetic/Parasympathetic • Abdominal Guarding
• Saliva Pooling Index • Autonomic Tone • Hydration Baselines
The system will calculate this index by monitoring three main areas:
A. Airway Safety (Target: ≥ 85/100)
The system will monitor how well a child coordinates swallowing and breathing.
- Swallowing Alignment: In a stable body, swallowing should happen when a child is breathing out. Future software will track this using chest-movement cameras and throat microphones. If a child frequently swallows while breathing in, the safety score will drop.
- Throat Audio Monitoring: Audio sensors will listen for micro-choking, wet hoarseness, or gurgling. A sudden increase in fluid sounds will flag that fluid is pooling in the throat.
B. Nervous System Balance (Target: ≥ 80/100)
The system will measure the balance between the body’s “fight-or-flight” stress response and its “rest-and-digest” recovery response.
- Heart Rate Variability (HRV): The software will monitor heart rate patterns. A sudden, sharp drop in HRV below the child’s usual average will indicate the body is entering a state of physical panic or distress.
- Eye Tracking: Cameras will track real-time changes in pupil size. Constant dilated pupils under normal room lighting will reveal that the child’s nervous system is stuck in an invisible stress loop.
C. Digestive and Energy Reserves (Target: ≥ 90/100)
The system will track gut comfort, daily energy use, and sleep quality.
- Pain Detection: The software will look for specific facial expressions (like lowered eyebrows or wrinkled noses) combined with body movements like arching the back, which point to hidden reflux pain or gut cramping.
- Nighttime Oxygen: The system will look at sleep data. If a child’s oxygen levels drop below 92% several times an hour during sleep, the software will automatically lower the child’s daytime training targets by 40% to account for their exhaustion.
5. Non-Invasive Ways to Stabilize the Body
Traditional clinical interventions for severe airway and GI issues frequently rely on highly invasive surgeries, such as permanent tracheostomies, or gastric fundoplications. From a Dynamic Systems perspective, these invasive choices insert destructive disruptions into the child’s emerging sensory-motor framework, introduce recurrent infection risks, and cause a rapid decline in overall development.
Instead, Step Zero outlines a plan to attempt to achieve physical stability first using targeted, non-invasive therapies that do not cause brain fog or heavy sedation. Only if these fail, should more aggressive approaches be considered.
[ STEP ZERO NON-INVASIVE TECH STACK ]
├── AIRWAY ──> 0.01% Mucoadhesive Atropine Gel ───> Local Drying / Safe Airway Patency
├── GUT ──> Linaclotide / Prucalopride ─────────> Clears Gut / Eliminates Pain Spikes
└── SLEEP ──> Long-Term Non-Invasive Vent (CPAP) ─> Protects Nocturnal Oxygenation
1.) Airway Safety (0.01% Mucoadhesive Atropine Oral Gel): Standard oral medications for drooling circulate through the whole body, causing racing heart rates, heavy sedation, and confusion. We propose using a targeted 0.01% atropine gel applied directly inside the mouth. It stays on the oral tissue, working right at the salivary glands. This dries the mouth locally to protect the airway without causing the systemic side effects that block learning.
2.) Gut Comfort (Targeted Medications): Nerve damage in severe CP/HIE often causes stomach paralysis and severe constipation, leading to intense pain spikes. Older stomach drugs can enter the brain and cause unwanted movement side effects. We propose using newer, localized medications like Linaclotide or Prucalopride. These work entirely within the intestines to clear the gut and reduce pain, without ever entering the brain or causing extra drooling.
3.) Restoring Energy (Non-Invasive Ventilation): To protect a child’s daily energy, Step Zero suggests using nocturnal CPAP or BiPAP with gentle nasal masks. This prevents the airway from closing during deep sleep, eliminates hidden sleep apnea, and stabilizes oxygen. It stops the nighttime panic response, letting the child wake up with full energy and a brain that is ready for daytime learning.
6. Scientific Authority & Quality Assurance Validation
As per the Horizon Filter process, the latest professional research will be evaluated on a weekly basis and the recommendations of medications and devices will be regularly updated against current pediatric pulmonology and gastroenterology guidelines to ensure the NeuroLoop Protocol always reflects the safest medical evidence.
References
- Thelen, E., & Smith, L. B. (1994). A dynamic systems approach to the development of cognition and action. MIT Press.
- Parrot, M., Murphy, N., Rower, J. E., Reilly, C. A., Green, D., Tarrell, A., Watt, K., & Yellepeddi, V. (2026). Pediatric oral cavity physiologically based pharmacokinetic model to predict pharmacokinetics of mucoadhesive atropine gel to treat sialorrhea. Journal of Pharmacokinetics and Pharmacodynamics, 53(4), 29. PMID: 42243578
- Almohanna, S., Alanazi, N. F., AlGhamdi, M. A., & Halawani, M. (2026). Management of pediatric sialorrhea: A systematic review with a stepwise evidence-based clinical algorithm. International Journal of Pediatric Otorhinolaryngol, 207, 112887. PMID: 42242174
- Dev Med Child Neurol. (2026). Outcomes of children and young people with cerebral palsy receiving long-term respiratory support: A systematic review. Developmental Medicine & Child Neurology. PMID: 42218697
Author: Matt Palaszynski
- Founder, BRIGHT Foundation: Leading a global initiative to “close the loop” on Cerebral Palsy recovery through data-driven research.
- 25+ Years Lived Experience: Navigating life with a daughter with CP provides a primary, first-person understanding of the physiological and clinical gaps in current care models.
- GE Alumnus & Business Leader: Leveraging decades of experience in operational excellence, complex systems, and strategic leadership to apply rigorous meta-study frameworks to neurological research.
- Methodology: Combines personal advocacy with professional systems-thinking to synthesize NCBI PubMed data into the actionable NeuroLoop Protocol.
Conflict of Interest Statement
The BRIGHT Foundation and its founder, Matt Palaszynski, maintain no commercial or business interests in the medical technologies, pharmaceutical products, or clinical services discussed on this page.
- Non-Profit Mission: Our objective is purely research-driven, aimed at identifying the most effective paths to a functional cure.
- Independence: No funding is received from manufacturers of the devices or therapies reviewed in our weekly meta-studies.
- Transparency: All citations are linked directly to PubMed (PMIDs) to ensure users can verify the raw data independently.




