
Executive Summary: 34-Study Horizon Filter Evaluation Week 24, June 8th, 2026
A comprehensive evaluation of the 34-study batch confirms zero true Additive results capable of expanding the core engineering, software, or molecular architecture of the NeuroLoop Protocol. Instead, the literature falls entirely within the Supportive and Legacy perimeters.
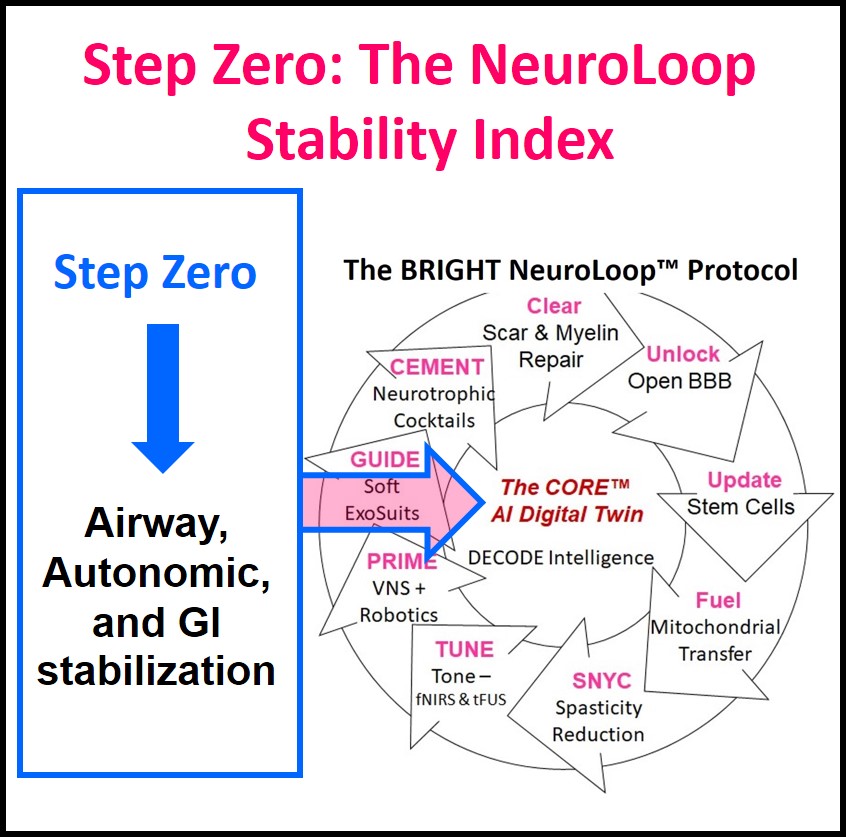
PROTOCOL UPDATE: “Step Zero: The NeuroLoop Stability Index“
However, Studies 17, 18, & 19 provided the critical mental push for BRIGHT to formally update the NeuroLoop Protocol, updating the protocol with “Step Zero: The NeuroLoop Stability Index” — a pre-protocol stabilization baseline.
For 25 years BRIGHT has tracked critical stability factors via its CP Repository data as well as intuitive inference from our own children. BRIGHT has called it the “Vicious Cycle of Brain Injury“: airway protection, the fight-or-flight reflex, and acid reflux combine to trigger harmful brain rewiring. The body remains trapped in a metabolic survival loop. Attempting to force surgical, or even neuroplastic, changes on an unstable biological platform triggers severe regression, secondary infections, and can ultimately lead to increased disability and even early death. (Examples are aggressive orthopedic surgeries, tracheotomies, etc.). Step Zero is now codified as the mandatory gateway that protects the child’s life and unlocks future neuroplasticity.
Study 17 & 18: Mucoadhesive atropine gel & Sialorrhea management algorithms (PMID: 42243578, PMID: 42242174)
- Analysis: Supportive. Managing sialorrhea solves secondary bulbar and airway issues, drastically reducing autonomic stress and baseline exhaustion.
Study 19: Long-term respiratory support outcomes (PMID: 42218697)
- Analysis: Supportive. Confirms that severe respiratory compromise exhausts metabolic baselines, validating the proximal-distal assertion that breathing costs subtract from motor bandwidth.
Supportive Insights (Studies 21, 22, & 29)
- Study 21 (Exoskeletons, PMID: 42226633) & Study 22 (AAC, PMID: 42223368): Classified as Supportive. They validate the biological targets of proximal unloading and alternative cortical capacity liberation, confirming mechanisms that the Core AI automates.
- Study 29 (Infant Wearable Accelerometry, PMID: 42243323): Strongly Supportive. It proves that high-frequency sensor data under 9 weeks of age successfully captures early motor abnormalities, validating the precise early-window data pipelines ingested by the NeuroLoop.
🔴The Stem Cell Null Result (Study 30, Mesenchymal Stromal Cells, PMID: 42241571)
- Referencing the NeuroLoop UPDATE Domain, Study 30 (Mesenchymal Stromal Cells, PMID: 42241571) is confirmed as a Null Result. While 4 infants with milder initial periventricular hemorrhagic injuries showed recovery, all five infants with severe injuries developed severe disabilities by age five. This explicitly indicates that the stem cells failed to reverse the initial underlying structural damage, reinforcing the reality that passive biological injections cannot substitute for active, closed-loop neuroplastic reorganization.
The Remaining Data Set
The remaining 27 papers are classified as Mildly Supportive or Legacy. They either review historical, manual orthopedic interventions that the Core AI replaces, or provide high-level epidemiological tracking that adds generic baseline context without altering active rehabilitation dynamics.
NeuroLoop Protocol Matrix: Rigorous Weekly Stratification – Week 24
Note: True Additive status is strictly reserved for research that alters or expands the software, hardware, or molecular architecture of the NeuroLoop Protocol. All other papers are classified as Supportive (validating known biological mechanisms or targets automated by BRIGHT) or Legacy (relying on slow, manual, or retrospective methods that the Core AI replaces).
⬛ Null Result Group
This study directly challenges current non-loop clinical paradigms by proving that passive structural interventions fail to reverse severe damage in long-term functional tracking.
|
Status |
Core Finding & Target Module |
PMID / Source |
|
Null Result |
Study 30 (Yang et al.) ➔ Fails to Support Neuroplastic Reorganization: Evaluates 5-year follow-up outcomes of Mesenchymal Stromal Cells for preterm periventricular hemorrhagic infarction. While 4 infants with milder initial insults showed recovery, all five infants with severe injuries developed severe disabilities by age five, demonstrating that cell therapy alone did not reverse or repair the initial underlying structural damage. |
PMID: 42241571 |
High-Utility Supportive Group
These studies directly validate or provide actionable clinical data for the newly codified STEP ZERO modules, or validate core targets automated by the NeuroLoop AI.
|
Status |
Core Finding & Target Module |
PMID / Source |
|
Supportive |
Studies 17 & 18 (Parrot / Almohanna) ➔ Supports STEP ZERO (Airway Patency): Validates a novel 0.01% mucoadhesive atropine gel and clinical algorithms to reduce sialorrhea and micro-aspiration, providing the non-invasive pharmacological pathway required to clear the airway baseline without triggering systemic autonomic or CNS side effects. |
PMID: 42243578 |
|
Supportive |
Study 19 (Systematic Review) ➔ Supports STEP ZERO (Airway Patency): Confirms that long-term non-invasive ventilation (LT-NIV) stabilizes breathing and eliminates nocturnal airway collapse, while highlighting a massive clinical data vacuum in standard medical literature regarding long-term respiratory tracking. |
PMID: 42218697 |
|
Supportive |
Study 29 (Alvarado et al.) ➔ Supports CORE AI (Sensory-Motor Ingress): Proves that high-frequency wearable accelerometry in infants under 9 weeks successfully catches early motor abnormalities, validating the automated sensor timelines ingested by the NeuroLoop. |
PMID: 42243323 |
|
Supportive |
Study 21 (Postol et al.) ➔ Supports CORE AI (Proximal Unloading): Compiles meta-analysis data confirming that wearable overground exoskeletons drastically optimize gait and balance by mechanically reducing proximal postural strain. |
PMID: 42226633 |
|
Supportive |
Study 22 (Binger et al.) ➔ Supports CORE AI (Cortical Liberation): Validates that augmentative generative language intervention effectively bypasses vocal-motor exhaustion, reinforcing the objective of reclaiming distal cognitive bandwidth. |
PMID: 42223368 |
Mildly Supportive Group
These studies offer complementary biological insights, secondary symptom management validation, or diagnostic tracking metrics without altering the core software or hardware engineering loop.
|
Status |
Core Finding & Target Module |
PMID / Source |
|
Mildly Supportive |
Study 1 (Implementation Strategies) ➔ Supports Upper Extremity Modules: Outlines clinical delivery strategies for early hand therapy, validating the critical timing of distal neuroplastic windows. |
PMID: 42234861 |
|
Mildly Supportive |
Study 3 (van Ossenbruggen et al.) ➔ Supports Clinical Target Mapping: Categorizes patient-defined hand-arm treatment goals, mapping the functional endpoints that the AI tracks. |
PMID: 42226630 |
|
Mildly Supportive |
Study 5 (Jacobs et al.) ➔ Supports Sensory Feedback Modules: Uses 3D motion analysis to explicitly map corrupted, ascending proprioceptive deficits stretching from the hip to the ankle. |
PMID: 42228362 |
|
Mildly Supportive |
Study 7 (Alexander et al.) ➔ Supports Patient Profiling Modules: Differentiates between-subject gait variability signatures in PVL versus perinatal stroke to help predict structural capacity boundaries. |
PMID: 42248590 |
|
Mildly Supportive |
Study 9 (Karlsson et al.) ➔ Supports Virtual Feedback Modules: Tracks engagement and ethics of extended reality (XR) systems, validating the use of immersive digital feedback environments. |
PMID: 42249712 |
|
Mildly Supportive |
Study 11 (Piersanti et al.) ➔ Supports Tissue Diagnostics: Confirms ultrasound elastography as an objective, non-invasive diagnostic modality for tracking macro peripheral muscle tissue stiffness changes over time. |
PMID: 42231359 |
|
Mildly Supportive |
Study 12 (Efkere et al.) ➔ Supports Reflex Training Modules: Evaluates backward downhill treadmill training following chemical spasticity blocks, capturing eccentric reflex loading responses. |
PMID: 42229287 |
|
Mildly Supportive |
Study 13 (Schlichting et al.) ➔ Supports Remote Ingress Modules: Validates the feasibility, motor performance tracking, and parent compliance of early telerehabilitation in infants aged 0-2 years. |
PMID: 42223296 |
|
Mildly Supportive |
Study 14 (Manikandan et al.) ➔ Supports Adult Capacity Tracking: Evaluates compliance and feasibility metrics of an online exercise programme (CP-EXCEL) to stabilize adult metabolic endurance baselines. |
PMID: 42227252 |
|
Mildly Supportive |
Study 15 (Caldes et al.) ➔ Supports Environmental Compliance Modules: Highlights how social determinants of health create external compounding variables that can disrupt daily therapeutic protocol execution. |
PMID: 42245843 |
|
Mildly Supportive |
Study 20 (Gaynetdinova et al.) ➔ Supports Cellular Optimization Modules: Explores systemic inflammation tracking and pharmacological neuroprotection (Mexidol) to prepare the cellular environment for rehabilitation. |
PMID: 42246529 |
|
Mildly Supportive |
Study 24 (Lin et al.) ➔ Supports Spasticity Baseline Profiling: Tracks long-term complications and safety governance of Intrathecal Baclofen (ITB) pumps used to suppress global spinal reflex inputs. |
PMID: 42240894 |
|
Mildly Supportive |
Study 26 (Nakashima et al.) ➔ Supports Cognitive Engine Modules: Validates a child-focused movement imagery scale, measuring internal cognitive motor-planning paths without physical muscular exhaust. |
PMID: 42227595 |
|
Mildly Supportive |
Study 27 (Ayala et al.) ➔ Supports Prenatal Protection Modules: Reviews magnesium sulfate clinical protocols designed to protect early embryonic cortical architecture before any protocol deployment. |
PMID: 42248515 |
|
Mildly Supportive |
Study 32 (Gardella et al.) ➔ Supports Macro Risk Modeling: Provides sex-based meta-analysis data confirming the persistent excess risk of cerebral palsy in males across gestational ages. |
PMID: 42226051 |
|
Mildly Supportive |
Study 34 (Ventura et al.) ➔ Supports Baseline Capacity Modeling: Tracks long-term cognitive and motor outcomes after fetal growth restriction, detailing the constraints of compromised neural baselines. |
PMID: 4222096 |
Legacy Group
These studies rely on slow, manual, retrospective, or purely structural/surgical interventions that do not target active neuroplasticity, all of which the Core AI ecosystem replaces or supersedes.
|
Status |
Core Finding & Target Module |
PMID / Source |
|
Legacy |
Study 2 (Ryland et al.) ➔ Superseded by Core AI Dynamic Tracking: Synthesizes surgical and non-surgical management of fixed forearm pronation deformities using isolated, mechanical techniques rather than addressing the real-time proximal drivers. |
PMID: 42234568 |
|
Legacy |
Study 4 (Tachibana et al.) ➔ Superseded by Core AI Computer Vision: Relies on manual, slow, retrospective radiological evaluations of skeletal maturation and hip migration percentages over age-related growth. |
PMID: 42228471 |
|
Legacy |
Study 6 (Kisel et al.) ➔ Superseded by Core AI Early Prevention: Reviews palliative, non-reconstructive, and salvage hip surgeries for severe subluxation and pain management rather than active motor loop retraining. |
PMID: 42227261 |
|
Legacy |
Study 8 (Gahukamble et al.) ➔ Superseded by Core AI Predictive Modeling: Tracks recurrence rates and bone remodeling following invasive, fixed mechanical distal femoral extension osteotomies. |
PMID: 42228457 |
|
Legacy |
Study 16 (Chambers Commentary) ➔ Superseded by Core AI Functional Monitoring: Critique of traditional, manual, impairment-focused medical systems, calling for a pivot to child-centered tracking that the Core AI already automates. |
PMID: 42246756 |
|
Legacy |
Study 23 (Sinkala et al.) ➔ Superseded by Core AI Digital Ledger: Analyzes historical, slow, manual paper record reviews and retrospective documentation patterns in international clinical teaching environments. |
PMID: 42243818 |
|
Legacy |
Study 25 (Zafari et al.) ➔ Superseded by Core AI Real-Time Ingress: Evaluates historical birth trends and macro-demographic risk indicators utilizing slow, retrospective population registries in Norway. |
PMID: 42237791 |
|
Legacy |
Study 28 (Ramaswamy et al.) ➔ Superseded by Core AI Care Automation: Outlines standard, manual family-centered care coordination methods, which are replaced by automated digital coordination within the AI environment. |
PMID: 42236132 |
|
Legacy |
Study 31 (Størdal Commentary) ➔ Superseded by Core AI Macro Epidemiology: Focuses on high-level, retrospective clinical commentary tracking historical public health prevention guidelines. |
PMID: 42237794 |
|
Legacy |
Study 33 (Shakhshir et al.) ➔ Superseded by Core AI Diagnostic Modeling: Synthesizes historical, retrospective database reviews to link prenatal asthma medications with broad educational and developmental difficulties. |
PMID: 42224295 |
Glossary of Terms: Additive & Supportive Studies
This glossary defines the critical mechanisms, neurological concepts, and technical modules utilized across the Additive and Supportive studies within the NeuroLoop Protocol framework.
Step Zero Modules & Technical Metrics
- STEP ZERO (Autonomic & Airway Stabilization)
The foundational, non-negotiable architectural phase of the NeuroLoop Protocol. It requires the absolute stabilization of a child’s airway, breathing, and gastrointestinal comfort using non-invasive methods before any active motor training can begin. - NeuroLoop Stability Index (NL-SI)
A proprietary, real-time composite safety metric generated by the Core AI. It continuously cross-references a user’s airway patency, heart rate variability, and metabolic reserves to ensure the biological platform is stable enough to permit neuroplastic learning without triggering systemic regression. - Airway Patency Module
The technical tracking layer within the Core AI that monitors swallow frequency, laryngeal acoustics, and saliva pooling. It guides targeted, non-invasive interventions—such as mucoadhesive atropine gel—to prevent micro-aspiration and choking. - Mucoadhesive Polymer Matrix
A specialized drug-delivery formulation that physically binds to the wet mucosal lining of the oral cavity. In Step Zero, it is used to deliver micro-doses of atropine locally to salivary glands, maximizing local drying while preventing the systemic “dosing spikes” and central nervous system noise caused by traditional swallowed medications. - Anticholinergic Side Effects
The systemic adverse reactions (such as rapid heart rate, blurred vision, constipation, and sedation) caused by traditional oral drooling medications like glycopyrrolate. These side effects inject heavy neurological noise into the body, which the NeuroLoop explicitly avoids by utilizing localized delivery systems. - Long-Term Non-Invasive Ventilation (LT-NIV)
The use of external breathing support, such as Continuous Positive Airway Pressure (CPAP), without utilizing invasive surgical tubes (like tracheostomies). In Step Zero, LT-NIV stabilizes nocturnal breathing, eliminates airway collapse, and prevents the metabolic exhaustion that drains a child’s day-time cortical capacity.
Core AI & Neuroplastic Architecture Modules
- CORE AI (Central Processing & Cortical Reallocation)
The central intelligence engine of the NeuroLoop Protocol. It ingests high-frequency data from computer vision and wearable sensors to dynamically calculate, adapt, and automate customized physical training loops optimized for active neuroplasticity. - Proximal-Distal Law
The neurobiological principle stating that the intense muscle effort required to hold up the core body (proximal) against gravity exhausts a child’s available brain power (cortical capacity). This survival-level exhaustion directly robs the brain of the bandwidth needed to control speech, swallowing, and fine finger movements (distal). - Proximal Unloading Module
The software and hardware control loop that handles the mechanical reduction of postural strain. By automating or tracking the use of supportive devices like overground exoskeletons, it lifts the burden off organic proximal muscles to instantly free up cortical bandwidth for distal motor tasks. - Cortical Capacity Liberation
The primary goal of the NeuroLoop Protocol. It is the process of reclaiming trapped brain bandwidth by systematically eliminating airway stress, visceral pain, and postural exhaust, allowing the primary motor cortex to focus entirely on learning new functional movement pathways. - Sensory-Motor Ingress Module
The data pipeline within the Core AI that continuously ingests and decodes high-frequency movement metrics from wearable sensors (such as infant accelerometers) and real-time computer vision streams to build an objective map of a child’s kinetic baseline. - Dynamic Systems Theory (DST)
A framework in developmental psychology and physics viewing human movement as a complex, self-organizing system where the brain, the body, and the environment are entirely interconnected. Under DST, a change in one boundary condition (like reducing gut pain or drying up saliva pooling) immediately reshapes the behavior of the entire motor system.
Adjacent Biological & Feedback Subsystems
- Heart Rate Variability (HRV)
The specific mathematical variation in time intervals between consecutive heartbeats. The Core AI tracks HRV metrics (such as RMSSD) as a real-time proxy for the autonomic nervous system, ensuring the child remains in a relaxed, receptive neuroplastic state rather than a sympathetic “fight-or-flight” survival state. - Proprioceptive Deficits
A corruption in the body’s internal GPS system, where damage to the nervous system prevents ascending sensory loops from accurately reporting joint position, weight, and movement back to the brain. - Gait Variability Signatures
The unique, measurable fluctuations in walking patterns across successive steps. The Core AI profiles these signatures to differentiate between distinct underlying brain lesion types (such as Periventricular Leukomalacia versus Perinatal Stroke) to accurately predict a child’s baseline capacity boundaries. - Movement Imagery / Motor Imagery
The active cognitive practice of visualizing a specific physical movement in the mind without actually contracting the physical muscles. This process activates the pre-motor and primary motor cortices, allowing for cognitive motor planning and training without causing physical muscular fatigue or metabolic exhaust. - Visceral Pain Response
The intense, deep-seated pain signaling originating from internal organs, primarily caused by gastrointestinal issues like severe reflux or delayed stomach emptying. In severe cerebral palsy, this unmanaged internal pain triggers massive sympathetic cortisol spikes that completely derail active motor learning.
Creator Credentials
Author: Matt Palaszynski
- Founder, BRIGHT Foundation: Leading a global initiative to “close the loop” on Cerebral Palsy recovery through data-driven research.
- 25+ Years Lived Experience: Navigating life with a daughter with CP provides a primary, first-person understanding of the physiological and clinical gaps in current care models.
- GE Alumnus & Business Leader: Leveraging decades of experience in operational excellence, complex systems, and strategic leadership to apply rigorous meta-study frameworks to neurological research.
- Methodology: Combines personal advocacy with professional systems-thinking to synthesize NCBI PubMed data into the actionable NeuroLoop Protocol.
Conflict of Interest Statement
The BRIGHT Foundation and its founder, Matt Palaszynski, maintain no commercial or business interests in the medical technologies, pharmaceutical products, or clinical services discussed on this page.
- Non-Profit Mission: Our objective is purely research-driven, aimed at identifying the most effective paths to a functional cure.
- Independence: No funding is received from manufacturers of the devices or therapies reviewed in our weekly meta-studies.
- Transparency: All citations are linked directly to PubMed (PMIDs) to ensure users can verify the raw data independently.




